

Author: Sharanya Seth
Mentor: Dr Zion Tse
United World College South East Asia
Abstract
The field of bionic limb technology is currently undergoing a pivotal paradigm shift, transitioning from purely functional robotic design to highly integrated neuroprosthetic systems. While contemporary advancements in neural interfaces and powered robotics have improved user capabilities, clinical translation remains hampered by issues such as signal instability, limited sensory feedback, and poor biocompatibility of interfaces. This literature review synthesizes recent progress in the clinical translation of bionic limbs, focusing on three core pillars: advanced neural interfaces, osseointegration, and patient-centric design. We explore the role of bidirectional control, the application of reinforcement learning for robust intent decoding, and the integration of digital twins for personalised residuum management. By evaluating the co-evolution of surgical innovation and robotic hardware, this review highlights the critical need for a “clinical-push” methodology, in which design is driven by long-term residuum health rather than mere functional performance. The findings emphasise that successful clinical outcomes depend on treating the prosthetic and the user’s altered physiology as a single, integrated system, ultimately identifying key barriers to translation and proposing a framework for more equitable, accessible, and durable prosthetic care.
Keywords: Neuroprosthesis, Bionic Limbs, Neural Interfaces, Osseointegration, Rehabilitation, Neuroplasticity, Bidirectional, Targetted Muscle Reinnervation (TMR), and Agonist-Antagonist Myoneural Interface (AMI)
1. Introduction:
The cinematic image of a sophisticated, seamlessly integrated artificial limb, once a domain of science fiction, is slowly becoming a clinical reality. For centuries, the ambition to replace missing limbs with functional, anthropomorphic counterparts has driven immense innovation. Yet, the reality of many amputees remains defined by the limitations of traditional, socket-based prostheses. While these conventional devices provide basic mobility, they are frequently associated with chronic pain, skin breakdown, and osseous degeneration, leading to high rates of device abandonment. The core of this challenge lies in the “HMI paradox” whereby, as the level of amputation increases, the technical complexity required for control increases as well, while the available biological signals from the residual limb diminish.
To overcome these barriers, the field has increasingly turned towards bionic limbs, which aim to replicate biological function through a marriage of robotics, surgery, and neuroscience. Unlike passive devices, modern bionic limbs leverage sophisticated neural interfaces, such as Targeted Muscle Reinnervation (TMR) and the Agonist-Antagonist Myoneural Interface (AMI), to create direct channels for motor intent and sensory feedback. Furthermore, the emergence of osseointegration, where prosthetics are directly skeletally attached, offers a stable, reliable foundation that bypasses the limitation of soft-tissue socket interfaces entirely.
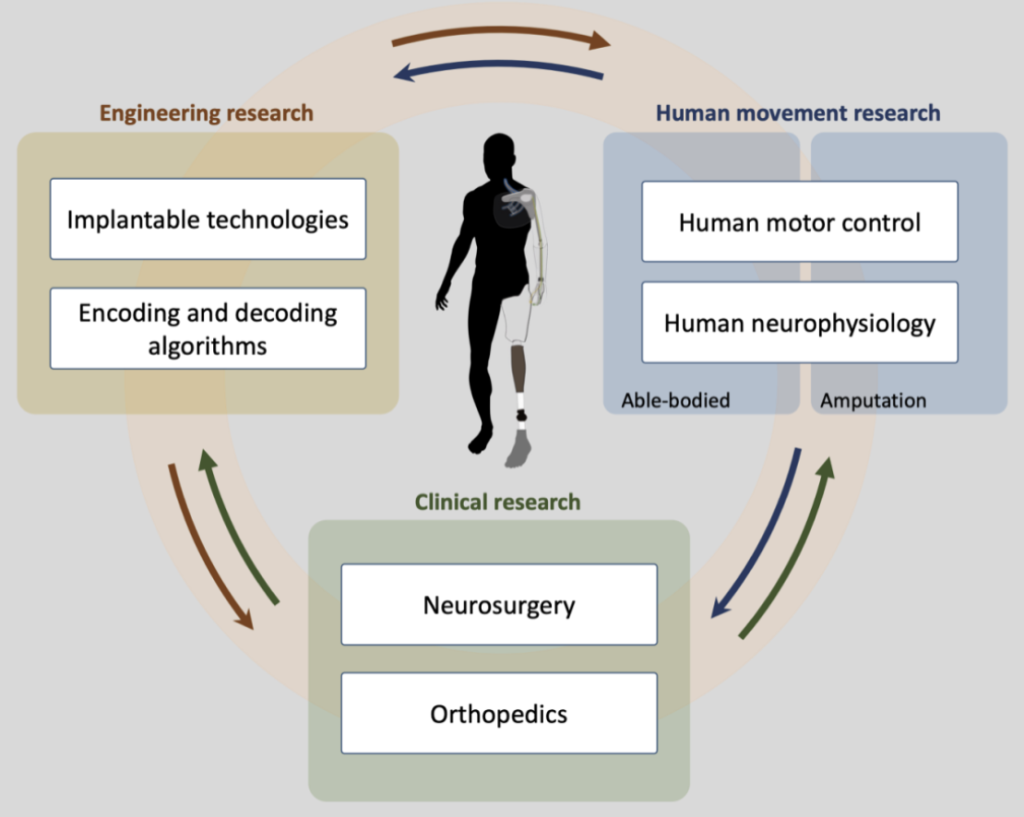
However, technology alone does not guarantee success. The history of prosthetic development has been dominated by a “technological-push” model, often neglecting the biological reality of the user. True clinical translation requires a transition toward a patient-centric approach that prioritises residuum health, embodiment, and long-term viability (Figure 1). This literature review examines the intersection of three fundamental domains: neural interfaces, which bridge the gap between brain and machine; osseointegration, which ensures skeletal and functional stability; and patient-centric design, which integrates digital monitoring and personalised rehabilitation (Figure 1). In the following sections, I will synthesise these advancements, starting with the technical evolution of bidirectional neural control, moving into the essential role of skeletal integration and residuum health, and concluding with a framework for how researchers may overcome current clinical and organisational barriers to make bionic limbs a sustainable, equitable standard of care.
2. Neural Interfaces and Bidirectional Control
Establishing a reliable, bidirectional link with the peripheral nervous system serves as the foundational requirement for any functional bionic limb. Recent surgical breakthroughs seek to maximise the “information throughput” of this interface, ensuring that the human-machine interaction is not limited by a lack of viable control signals.
Amputations affect hundreds of thousands of people each year in the United States and Europe, particularly. Therefore, there has been a growing interest in neuroprosthetics that can restore both movement and sensation. While today’s bionic limbs can perform increasingly precise movements, they still fall relatively short when replicating a natural limb. One of the biggest challenges regarding this is establishing a strong, long-term connection with the peripheral nervous system that can both monitor motor commands and deliver meaningful sensory feedback (Cho et al., 2023). Existing neural interfaces, whether engineered or biological solutions, often struggle with durability, biocompatibility, and limited signal variety. A new hybrid bionic interface has been established to bridge these gaps by combining a regenerative peripheral nerve interface (RPNI) with a traditional nerve interface with a single implant (Cho et al., 2023). The device uses a buckle-shaped design made from a shape memory polymer (SMP), allowing it to be easily implanted onto a severed nerve while also connecting to a muscle graft. Long-term in rabbits showed that the interface remained stable and biocompatible while reliably recording and stimulating neural signals (Cho et al., 2023). Most importantly, it was able to capture distinct motor signals during natural walking and use as a robotic leg. Overall, the hybrid interface offers a more flexible and information-rich way to connect nerves to prosthetics, bringing neuroprosthetic control closer to natural movement and sensation.
2.1 Continuous Neural Control of a Bionic Limb
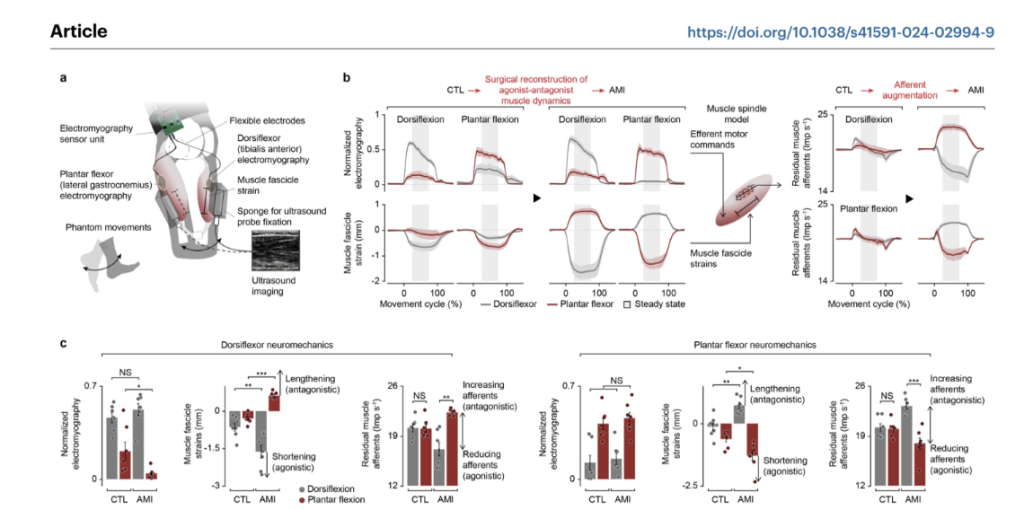
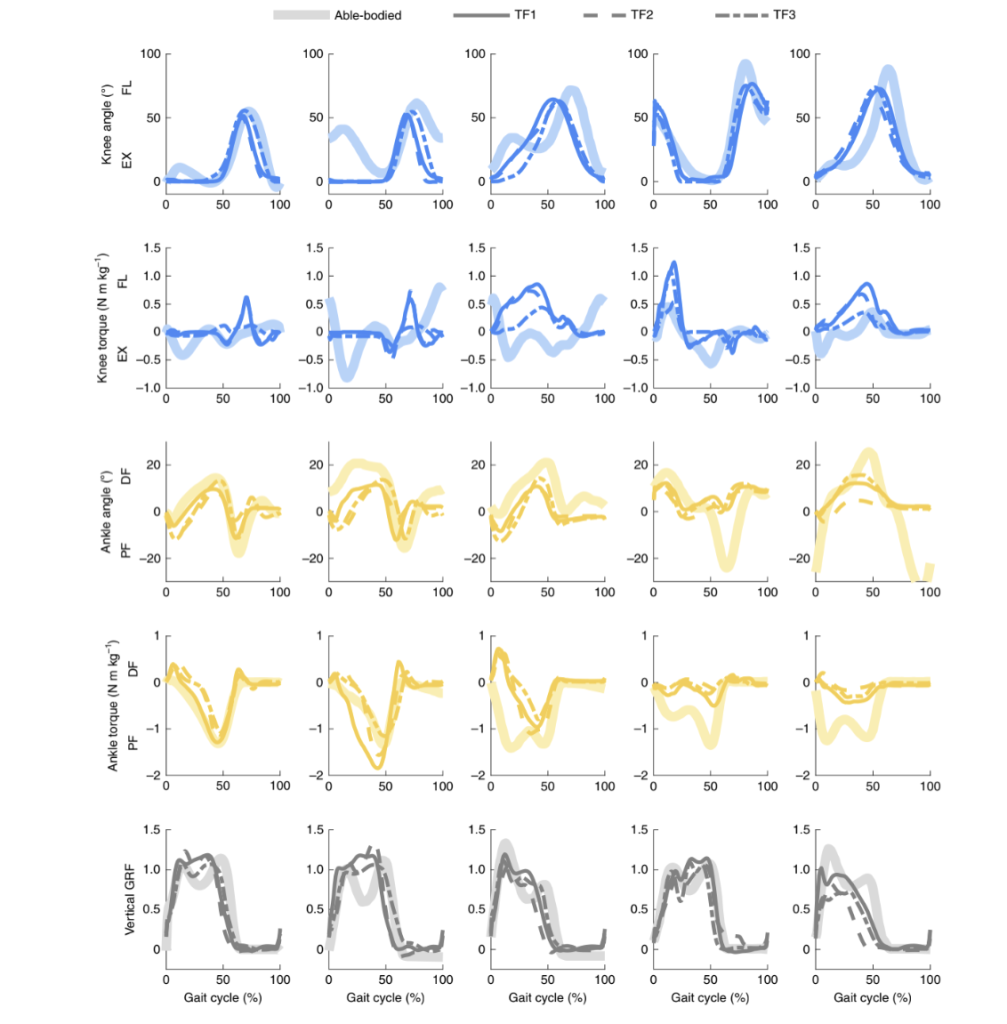
A 2024 study in Nature Medicine highlights a significant paradigm shift in prosthetic technology by prioritising surgical-neural integration through the Agonist-Antagonist Myoneural Interface (AMI) (Song et al., 2024). Unlike contemporary bionic limbs that rely on intrinsic pre-defined control frameworks to estimate gait phases, the AMI procedure restores a degree of natural proprioception by surgically reconnecting residual muscle pairs. This interface allows the human nervous system to directly and continuously neuromodulate the bionic limb (Figure 2), augmenting residual muscle afferents by 18% if biologically intact values (Song et al., 2024). This restoration of sensory feedback proved sufficient to enable a highly biomimetic gait, with participants achieving a 41% increase in maximum walking speed compared to matched control cohorts (Song et al., 2024). Furthermore, the study demonstrates that this level of afferent augmentation allows for seamless adaptation to complex, real-world environments such as stairs, slopes, and obstructed pathways without the need for robotic decision-making (Figure 2). Ultimately, these results suggest that even partial reinstatement of the biological feedback loop is sufficient for the human nervous system to regain versatile, biomimetic motor control, offering a potent alternative to autonomous robotic systems.
2.2 Improving Bionic Limb Control
Freitag et al. (2026) investigated the use of reinforced learning (RL) to improve the decoding of human motor intent for bionic limb control using electromyographic signals (EMG) (Freitag et al., 2026). Accurate and robust intent decoding remains a major challenge in prosthetics, and most existing approaches rely on supervised learning (SL) trained on static, labeled EMG datasets (Freitag et al., 2026). However, such data fails to reflect natural muscle activity during real-world use, limiting online performance and usability. The researchers propose a novel training framework that combines SL and RL. An initial control policy is first pretrained using supervised learning based on EMG recordings. This policy is fine-tuned using offline reinforcement learning with dynamic EMG data collected while participants interact with a custom-designed, Guitar Hero-inspired game. The game environment enables real-time, human-in-the-loop interaction and provides a structured reward signal based on movement accuracy and timing. The Advantage Weighted Actor Critic (AWAC) algorithm is used to improve the policy while remaining close to previously learned behaviours (Freitag et al., 2026). Experiments were conducted with nine able-bodied participants performing simultaneous finger movements. Results show a threefold increase in normalized cumulative reward and more than a two-fold improvement in decoding accuracy compared to the supervised baseline (Freitag et al, 2026). Improvements generalised to a separate motion test, demonstrating enhanced robustness. The study concluded that reinforcement learning on interactive, usage-based data can bridge the gap between offline training and real-world prosthetic control, supporting more intuitive and reliable bionic limb operation.
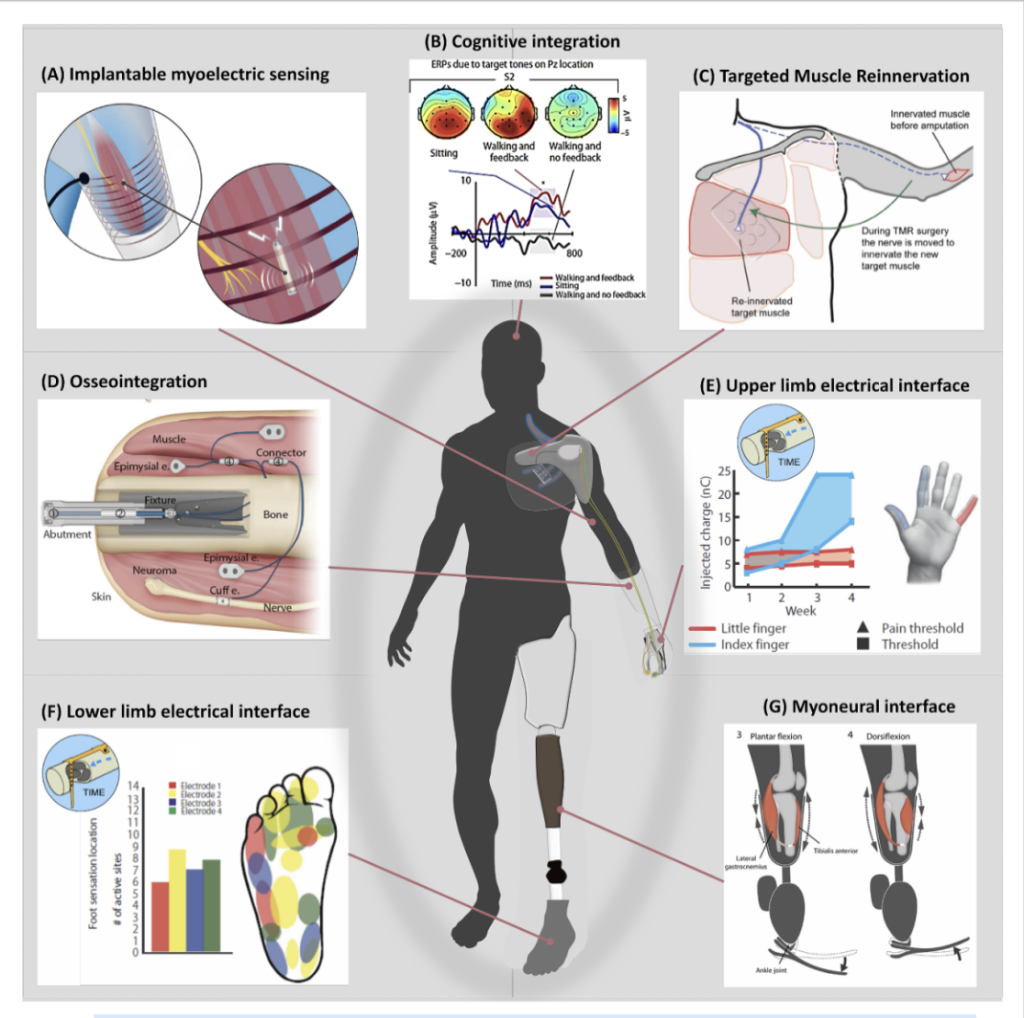
The future of bionic limbs depends on bridging the gap between advanced engineering and the biological reality of the post-amputation physiology of patients (Paslausta et al., 2022). Engineers have developed sophisticated bidirectional systems capable of decoding motor intent and providing sensor feedback using surgical techniques like Targeted Muscle Reinnervation (TMR) and Agonist-Antagonist Myoneural Interface (AMI) (Paslausta et al., 2022) (Figure 3). Methods like TMR and AMI are highlighted for their ability to recreate biological feedback loops, such as proprioception, that the brain expects to receive (Figure 3). Moreover, researchers highlight the need for biomimetic encoding and moving beyond simple electrical pulses to natural sensory algorithms with a deeper focus on motor control theory and understanding how the brain manages postural balance and embodiment (Paslausta et al., 2022).
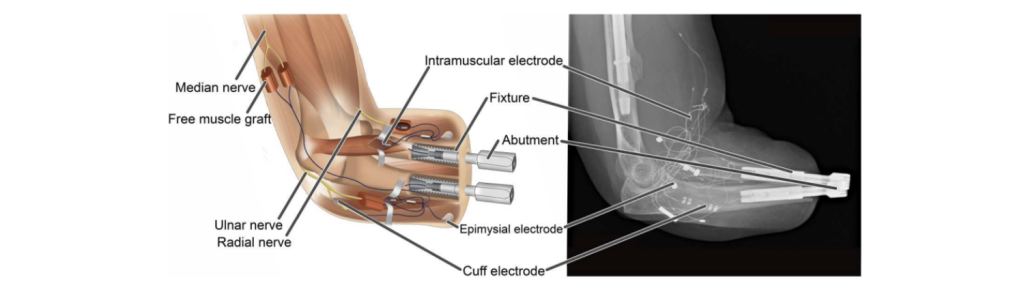
Restoration of sensorimotor function in upper limb amputees has historically been limited by the lack of reliable control, sensory feedback, and comfortable attachment (Ortiz-Catalan et al., 2023). Traditional socket-based prostheses often cause discomfort and rely on surface electrodes that are prone to signal interference. Ortiz-Catalan et al. detail the clinical implementation of a transradial neuromusculoskeletal prosthesis, which connects a bionic hand directly to the user’s nervous and skeletal systems (Figure 4). In a landmark case study, a patient with a below-elbow amputation received titanium implants in the radius and ulna for osseointegration, providing stable skeletal attachment (Figure 4). Surgically, the interface was enhanced by creating regenerative peripheral nerve interfaces (RPNIs) through the transfer of severed nerves into free muscle grafts (Ortiz-Catalan et al., 2023). These grafts, along with native muscles and the ulnar nerve, were instrumented with implanted electrodes (Figure 4). The resulting system is entirely self-contained, requiring no external batteries or processing units for daily use.
Long-term results over three years demonstrated significant improvements:
- Enhanced Function: Improved scores in the Southampton Hand Assessment Procedure (SHAP) and Assessment of Capacity for Myoelectric Control (ACMC).
- Sensory Feedback: Consistent tactile sensations elicited via direct neural stimulation of the ulnar nerve.
- Quality of Life: A marked reduction in phantom limb pain and a substantial increase in overall well-being.
This integrated approach overcomes the “HMI paradox” by providing a high-bandwidth, stable, and bidirectional communication channel between the patient and the bionic limb (Ortiz-Catalan et al., 2023).
3. Neuroplasticity and User Adaptation
Once a physical neural connection is achieved, the focus must shift to the central nervous”s systems” innate ability to adapt to artificial input. Understanding the brain’s capacity for cortical reorganisation is essential, as the user must essentially re-learn how to control a limb that no longer communicates through the traditional biological pathways.
3.1 Bidirectional Bionic Limbs
Although engineers have developed sophisticated bidirectional systems capable of decoding motor intent and providing sensory feedback, these technologies often operate in a vacuum, failing to account for how nervous systems reshape after losing a limb (Paslausta et al., 2022). Amputation triggers significant cortical reorganisation, where the brain’s sensory and motor maps may shrink or shift over time (Paslausta et al., 2022). To address this, a transdisciplinary approach is required to manage neuroplasticity. Thus, a solution that combines high-tech hardware with innovative surgical techniques must be implemented. Ultimately, restoring the true function of a missing limb requires treating the prosthesis and the patient’s altered physiology as a single, integrated system rather than separate components (Paslausta et al., 2022).
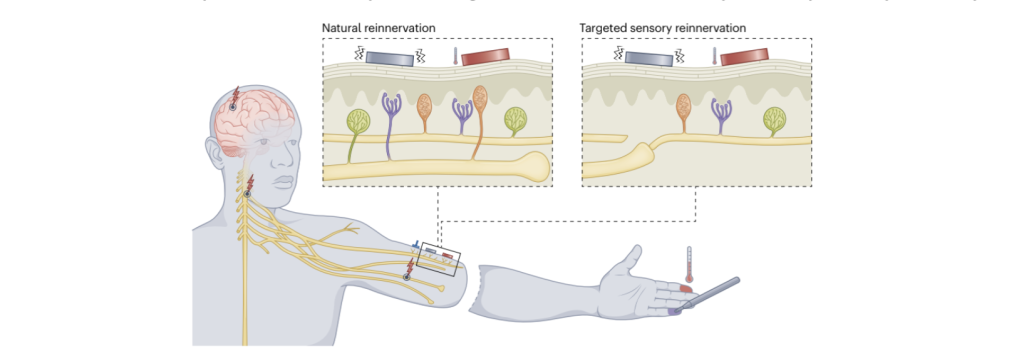
The concurrent TMR, targeted sensory reinnervation (TSR) for touch, and vibration-induced kinesthesia significantly advance bionic limb functionality toward able-bodied norms (Marasco et al., 2021) (Figure 5). By establishing a bidirectional neural-machine interface in participants with proximal neural-limb amputations, this approach moves beyond traditional myoelectric control to restore complex sensory-motor loops. The simultaneous delivery of tactile and kinesthetic feedback allows users to transition from speed-driven, compensatory behaviours to accuracy-maximising strategies, characterised by a marked reduction in visual dependency (Marasco et al., 2021). This restoration of feedback channels promotes a measurable shift in visuomotor behaviour whereby users redirect their gaze from the prosthetic hand toward the intended target while also enhancing limb ownership by aligning the device’s performance with the brain’s internal model (Marasco et al., 2021) (Figure 5). Ultimately, providing a multifaceted sensory experience is critical for reducing cognitive load and achieving “human-like” integration in prosthetic systems, effectively stratifying bionic performance away from conventional prosthetics and toward natural physiological function.
3.2 Biometric Versus Arbitrary Motor Control
Contrary to the long-standing “biomimetic assumption” in neuroprosthetics, recent evidence from Nature Human Behaviour (2024) suggests that anthropomorphic control strategies, those that mimic biological movements, do not inherently provide superior long-term benefit for device learning or embodiment (Schone et al., 2024). By evaluating participants using a myoelectric bionic hand, researchers compared a biomimetic mapping against an arbitrary, non-biomimetic strategy to determine if recruiting pre-existing neural resources actually enhances performance. The findings revealed that while biomimetic control offered an initial “intuitive” advantage in speed and automaticity, these differences vanished as training progressed, with arbitrary users eventually matching their counterparts in dexterity and gesture switching (Marasco et al., 2021). The study further demonstrated that the arbitrary control group exhibited significantly higher levels of generalisation when they were tasked with a novel control mapping; arbitrary users maintained their proficiency, whereas biomimetic users experienced a sharp decline in performance (Marasco et al., 2021). Interestingly, both groups reported significant and comparable increases in a sense of embodiment, specifically regarding agency and body ownership, thus indicating that the bian’s integration of the tool depends more on the reliability of the human-machine interface than on anatomical mimicry. These results suggest that by moving away from strict biomimicry, designers can leverage the nervous system’s capacity for reinforcement learning to create more flexible, functional, and adaptable prosthetic solutions.
4. Osseointegration and Skeletal Integration
While neural signals provide the intent, the physical stability of the limb is what allows that intent to be translated into meaningful action. Osseointegration represents a landmark advancement in this regard, moving away from adverse effects and issues of traditional sockets toward a permanent, bone-anchored skeletal attachment.
Traditional socket-based prostheses frequently cause discomfort, skin damage, and limited mobility, often resulting in high rates of device abandonment (Frossard and Lloyd, 2021). In contrast, osseointegrated bionic limbs are directly anchored to the bone, offering significantly improved stability and mobility (Frossard and Lloyd, 2021). This direct connection facilitates “osseoperception”, a form of sensory feedback that allows users to walk more naturally and experience an enhanced sense of embodiment (Frossard and Lloyd, 2021). By providing a stable mechanical foundation, osseointegration overcomes the functional limitations of the soft-tissue interface.
Azocar et al. researched the design, implementation, and clinical testing of the Open Source Leg (OSL), an integrated robotic knee-ankle prosthesis developed to advance research and clinical evaluation of powered lower limb prostheses in real-world environments (Figure 6). While powered prostheses can improve walking speed, stability, and energy efficiency for individuals, progress has been limited by high costs, proprietary designs, and the lack of standardized hardware for testing control strategies. The OSL addresses these challenges by providing a low-cost, portable, customisable, and fully open-source platform (Azocar et al., 2020). The prosthesis integrates high-torque electric motors, low-ratio belt transmissions, embedded sensing, and low-level control software, thus enabling independent operation of the knee and ankle joints (Azocar et al., 2020). A configurable series elastic actuator allows researchers to adjust joint stiffness and study different control options. Extensive benchtop testing demonstrated high bandwidth, accurate position and current control, reliable torque output, and safe thermal performance (Azocar et al., 2020). Clinical testing with 3 individuals with lower limb amputations showed that OSL supports stable ambulation across level ground, ramps, and stairs, using impedance-based control whereby participants achieved kinematics and kinetics comparable to able-bodied walking (Azocar et al., 2020) (Figure 6). By releasing hardware designs, software, and benchmark datasets, the OSL lowers barriers to prosthetic research and enables fair comparison of control strategies, supporting future innovation in bionic limb technology.
4.1 Bionic Limb Replacement
Amin (2022) examined the evolving role of bionic limb replacement in the context of lower extremity reconstruction. Advances in lower extremity reconstruction, including microvascular techniques, nerve and tendon transfers, and complex bone reconstruction, have expanded limb salvage options, but outcomes are still often limited by infection, unstable soft tissues, prolonged rehabilitation, chronic pain, and donor site morbidity. When salvage is unsuccessful, amputation with prosthetic fitting remains a common solution; however, conventional prosthetic fitting frequently fails to provide comfortable, efficient, and intuitive function, particularly due to issues with socket fit, increased energy expenditure, and lack of sensory feedback. Emerging bionic limb technologies offer a potential alternative by aiming to restore bidirectional communication between the nervous system and prosthetic devices (Amin, 2022). Approaches such as myoelectric control, targeted muscle reinnervation, and direct neural interfacing through extraneural, intraneural, and regenerative electrodes have demonstrated promise in improving motor control and sensory perception (Amin, 2020). Nevertheless, significant challenges remain, including signal instability, biological compatibility, invasiveness, and long-term reliability (Amin, 2020). Collectively, this body of work suggests that future progress in lower limb reconstruction will increasingly rely on interdisciplinary advances in neural interfaces, robotics, and tissue engineering to develop more functional and intuitive bionic limb replacements.
4.2 Self-Contained Bidirectional Bionic Limbs
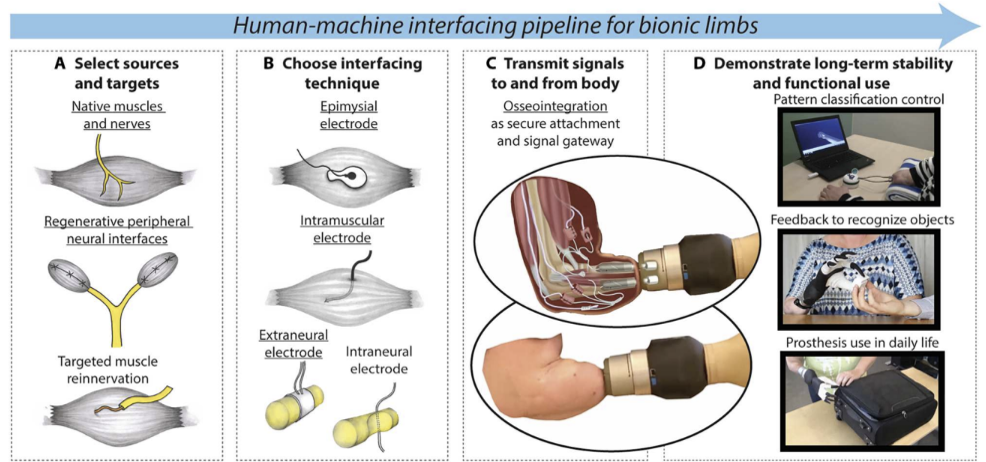
Surgical neural engineering and human-machine interfacing (HMI) have reached a milestone with the development of fully self-contained, bidirectional bionic limbs. A primary challenge in prosthetics is the “HMI paradox” whereby, as amputation levels rise, the complexity of the required prosthesis increases while the number of available biological control signals decreases (Dosen, 2023). To overcome this, a comprehensive HMI pipeline integrates advanced surgical techniques, such as muscle grafts and targeted muscle reinnervation, to create additional signal sources (Ortiz-Catalan et al., 2023). The system implemented by Ortiz – Catalan et al. utilises osseointegration, which is the permanent attachment of the prosthesis to the skeleton via titanium implants. This provides a stable gateway for bidirectional communication. Motor control is achieved through intramuscular and epimysial electrodes that record from native muscles and grafts, while sensory feedback is restored by delivering electrical stimulation to the ulnar nerves via extraneural cuff electrodes (Ortiz-Catalan et al., 2023). Long-term clinical results over three years demonstrate that this approach enables stable, dexterous control of individual digits and provides intuitive tactile sensations (Ortiz-Catalan et al., 2023). By combining skeletal attachment with implanted neural interfaces (Figure 7), this research moves closer to the ideal reality of bionic replacement: a limb that offers effortless, simultaneous control and natural somatosensory feedback, significantly enhancing the user’s daily quality of life.
5. Sensory Feedback and Embodiment
The ultimate success of a bionic limb is often defined by the user’s sense of ownership over the device, referred to as a psychological state known as embodiment. This state is achieved only when the brain receives consistent, multi-modal sensory feedback, such as heat, pressure, and kinesthesia, that aligns with its internal motor expectations.
5.1 Thermally Sentient Bionic Limbs
Ortiz-Catalan argued for exploring thermal sensation as an added sensory modality in bionic limbs through sensory reinnervation. When nerves from an amputated limb naturally or surgically reinnervate the skin of the residual limb, they create “phantom maps”. By stimulating these specific areas with compact thermoelectric devices, researchers successfully triggered sensations of heat and cold, localised by the brain to the missing upper limb (Ortiz-Catalan, 2024). Moreover, in clinical trials, participants were able to distinguish between different materials, such as copper or glass, and accurately identify the temperature of objects they made contact with while wearing the bionic limb (Ortiz-Catalan, 2024). Unlike electrical nerve stimulation, which often may feel artificial, thermal stimulation of the phantom maps feels natural because it activates biological sensors as intended (Ortiz-Catalan, 2024). However, these maps are often somatopically disorganized or incomplete, though remaining stable for 48 weeks (Ortiz-Catalan, 2024). Therefore, it does still offer a promising avenue for long-term research and daily use. Ultimately, while thermal sensing may enhance the bionic limb user’s sense of “embodiment”, its primary value lies in improving the functional and social capabilities of artificial limbs.
5.2 Bionic E-Skin
Xu et al. (2024) introduced a self-powered bionic droplet electronic skin (DES), designed to help bionic limbs establish a sense of touch to liquids (Figure 8). Generally, e-skins focus on solid pressure or temperatures, but most fail to perceive the movement of liquids. The proposed e-skin uses the triboelectric effect, meaning it generates its own electricity from the friction created when a water droplet slides across the surface, requiring no external power (Xu et al., 2024). This technological breakthrough is an interlaced electrode network and “overpass” connection design (Xu et al., 2024). This allows the skin to track the precise 2D trajectory, velocity, and acceleration of a droplet without the signal getting “crossed” or blurry. It’s so sensitive that it can even distinguish between different liquids such as tap water, rainwater, and seawater, based on their specific electrical signatures (Xu et al., 2024). Beyond just sensing, researchers demonstrated autonomous regulation similar to human neuromodulation (Xu et al., 2024). For example, when the skin detects a liquid leak, it can identify the direction of the flow and trigger an intelligent closed-loop system to shut a valve and stop the leak (Xu et al., 2024). Moreover, the e-skin is made of flexible, waterproof materials, and the AI allows for navigation and reaction to wet, unpredictable environments like rain or industrial spills as intuitively as a human would (Xu et al., 2024).
6. Patient-Centric Design and Residuum Health
A sustainable bionic solution must prioritize the long-term health of the residual limb, or residuum, above mere mechanical performance. By utilising predictive tools such as digital twins, clinicians can now proactively manage the health of the patient’s tissue and bone, preventing the complications that historically led to prosthetic abandonment.
6.1 Advances in Clinical and Prosthetic Care
Frossard et al. (2022) highlighted the necessity of a critical shift in this field of medicine, moving beyond just building better AI to focus on the health of the residuum. Generally, prosthetics fail because of the adverse effects, such as skin issues, pain, and bone loss, caused by the interface between the body and the device. This leads to an increase in limb abandonment. To fix this, researchers are pushing “Bionic 4.0 solutions”: direct skeletal attachment, osseointegration, and advanced neural interfaces such as TMR to get rid of pain caused by sockets and to improve control while reducing phantom pain (Frossard et al., 2022). After surgery, rehab blueprints should be established with examples such as botulinum toxin to stop skin movement around implants and haptic sleeves that give users a sense of touch (Frossard et al., 2022). Furthermore, a healthy residuum is a multifaceted goal whereby the patient’s age, weight, and specific alignment of the prosthetic joint are all key factors, not just the surgery. Consequently, new technology such as the Computer Assisted Limb Assessment (CALA) allows clinicians to objectively map out patients’ phantom pain, thus making it easier to treat (Frossard et al., 2022). Overall, the goal should be to stop oscillation of patients between satisfactory mobility and bedridden pain by threatening the prosthesis and the patient’s biology as a single, connected system.
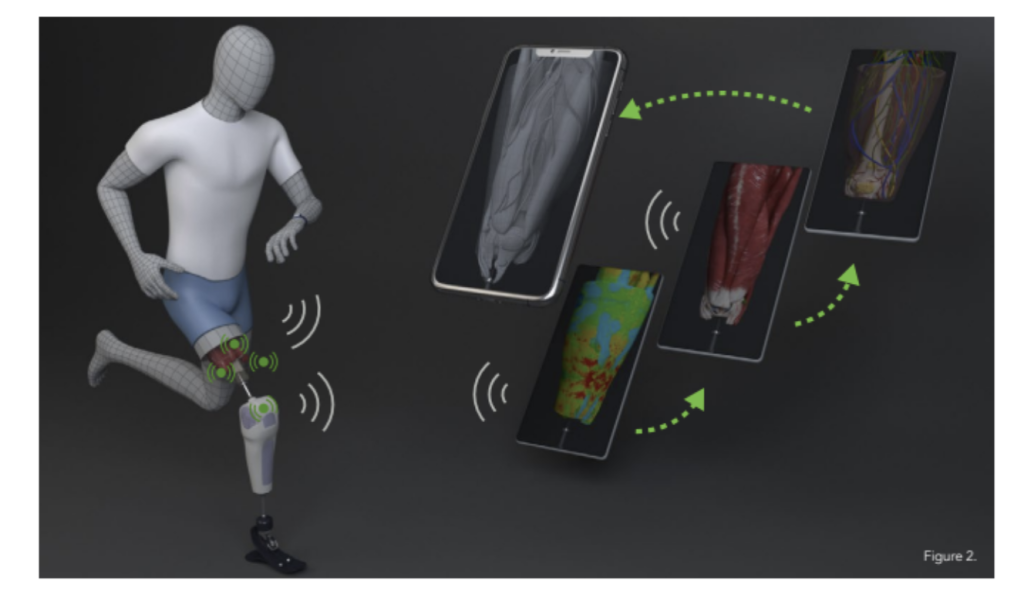
To address the risks associated with bone-anchored systems, such as infection, implant failure, and fractures, a novel and non-invasive diagnostic approach using a “digital twin” of the residuum was proposed by Frossard and Lloyd (2021). This high-fidelity, physics-based virtual model integrates real-time data from wearable sensors to monitor internal tissue response during prosthetic use (Frossard and Lloyd, 2021). By visualising stresses and movements within the limb, clinicians and patients can better manage loading patterns and reduce injury risk (Figure 8). This transformative step toward intelligent bionic limbs supports personalized rehabilitation and improves long-term patient safety.
7. Clinical Translation Challenges and Barriers
While laboratory milestones of the past decade are impressive, the transition from an experimental prototype to a standard-of-care medical device remains the most significant hurdle in prosthetic medicine. Evaluating bionic systems through a lens of translation-readiness reveals that high-performance metrics in a controlled setting do not always correlate with daily clinical utility. It is important to recognise that an ideal device in a lab may still fail in the real world if the surrounding infrastructure is not ready.
7.1 Technical Barriers: Reliability and Biotic-Abiotic Integration
The first layer of obstruction involves the physical and electrical longevity of the system. For a bionic limb to be truly translation-ready, it must move beyond “benchtop” success and demonstrate resilience against the unpredictability of human life. Biocompatibility remains a major concern; even the most advanced electrodes face the risk of signal instability and decay over time as the body’s foreign-body response encapsulates sensors in fibrous tissue (Amin, 2022). Furthermore, achieving a truly permanent solution requires overcoming the risks of chronic infection at the percutaneous interface, which is a significant hurdle for the long-term reliability of fully implantable systems (Bumbaširević, 2020). Additionally, maintaining stable closed-loop control is technically taxing outside of controlled laboratory environments, where external interference and extraneous variables may disrupt the delicate neural signals required for intuitive motor execution.
7.2 Clinical Organisation Barriers: The Infrastructure of Care
Advanced surgical interventions such as TMR or AMI require interdisciplinary teams that many regional clinics cannot support, leading to a disconnect between technological potential and actual clinical integration (Frossard et al., 2022). This disconnect is exacerbated by a reimbursement paradox: national health services and insurance providers are frequently hesitant to cover the high upfront costs of bionic limbs without longitudinal data proving they significantly reduce long-term secondary healthcare expenditures, such as caregiver reliance or mental health intervention. Without standardised clinical training and clear financial pathways, these innovations risk remaining research papers rather than becoming accessible medical standards.
7.3 Ethical and Equity Considerations: Democratising Innovation
Many current innovations are hindered by proprietary designs and “closed” software ecosystems that prevent interoperability between different manufacturers. This underscores a desperate need for standardised platforms that could lower production costs and facilitate broader distribution (Azocar et al., 2020).It also raises a critical question of equity, whereby if bionic limbs are only accessible to a small cohort of patients with premium insurance or specific military status, the field may inadvertently widen existing health disparities. An ethical transition toward “translation-readiness” must involve a shift from high-cost, exclusive prototypes toward inclusive, robust, and globally accessible bionic solutions.
8. Future Directions
While the preceding sections have outlined the state of the art and the barriers to implementation, the path forward requires a transition from demonstrating feasibility to ensuring longitudinal reliability. The next generation of research must prioritise the convergence of artificial intelligence, materials science, and standardised clinical protocols to transform bionic limbs from laboratory prototypes into lifelong biological extensions.
8.1 Technical Future: Intelligence and Sensation:
The technical evolution of bionics will likely focus on the development of more robust, long-term neural interfaces. Current evidence suggests a critical need for long-term human data to validate the stability of bidirectional communication over decades (Cho et al., 2023). Furthermore, the integration of ‘Reinforcement Learning’ (RL) must move beyond virtual simulations into real world settings, allowing devices to adapt dynamically to a user’s unique environment (Freitag et. al, 2026)Beyond motor control, the future lies in multi-modal feedback, incorporating thermally sentient capabilities and bionic e-skins to provide a nuanced sense of touch, temperature, and pressure (Ortiz-Catalan, 2024).
8.2 Clinical Future: Trials and Long-Term Outcomes
The clinical trajectory must shift toward larger trials and standardised long-term outcome measures. To ensure patient safety, future research should integrate residuum-centered protocols that monitor the health of the host tissue alongside device performance (Amin, 2022).This involves moving toward fully implantable systems that minimise the risk of infection while maximising signal fidelity.
8.3 Design and Policy Future: Equity and Standardisation
From a policy perspective, the field must address the “siloing” of technology. Moving away from proprietary designs toward standardised, adaptable platforms is essential for lowering costs and ensuring equitable access (Azocar et al., 2020). Future regulatory pathways must be streamlined to accelerate the transition from the “bench to the bedside”, ensuring that breakthroughs in the lab actually reach the diverse global population of limb loss patients.
8.4 Core Strategic Objectives:
- Small Learning Curves:
Future prosthetic design must prioritise intuitive control to minimise the cognitive burden on the patient. By aligning the device’s behaviour with the brain’s existing internal motor models, researchers can ensure that users do not require months of intensive training, making the technology accessible to a wider demographic regardless of technical proficiency.
- Simple Procedures for Insurance Coverage:
Clinical translation depends on moving toward surgical techniques that are standardised enough for general hospitals to perform. By simplifying the implementation of interfaces like TMR or AMI, the procedure becomes more “reimbursable” by insurance, shifting advanced bionics from an experimental luxury to a standard, covered medical necessity for all patients.
- Clinical Translation Focus:
The field must move away from “technological push” models toward a “clinical pull” strategy. This means prioritising the practical needs of the patient, such as the device weight, battery life, and skin comfort, over adding high-tech features that have little impact on daily quality of life or long-term functional independence in home environments.
- Integration of AI (System Thinking):
Rather than using AI for isolated tasks, future systems must adopt “system thinking” AI. This allows the limb to simultaneously manage motor intent, sensory feedback, and environmental adaptation. Instead of a one-size-fits-all functional design, AI will personalise the device’s response in real time, matching the specific physiological signatures of each individual user.
- Approval and Acceleration of Clinical Trials:
The primary bottleneck is no longer the technology itself, but the speed of regulatory approval. Accelerating the transition to large-scale clinical trials is the key to proving long-term safety and efficacy. Without these trials, even the most revolutionary designs will remain stuck in a “proof of concept” phase without reaching the public.
- Integration of Digital Twins:
Digital twins allow researchers to design and test prosthetics in a high-fidelity virtual environment before any surgery occurs. By simulating the interaction between the device and the patient’s unique bone and tissue structure, clinicians can perfect the design, predict potential failures, and minimise the risks of post-operative complications or revisions.
9. Conclusion
The evolution of bionic limb technology represents one of the most ambitious frontiers in modern medical engineering. As this review has demonstrated, the field has successfully moved beyond simple mechanical substitution toward a sophisticated model of neural and skeletal integration. However, the true measure of success for these innovations is not found in laboratory benchmarks or peak performance metrics, but in their capacity for meaningful clinical translation. For a bionic system to be effective, its design must be clinically driven, thus originating from the actual physiological and psychological needs of the patient rather than being a product of technological push, where features are added simply because they are technically possible.
The trajectory of a successful bionic innovation must follow a clear path: from the research bench, where fundamental science is born, to the clinical bedside, where the technology is safely and intuitively integrated into a patient’s life; and finally to the boardroom, where standardised manufacturing and insurance reimbursement models ensure the device is economically viable and globally accessible. By prioritising “system thinking” through AI and digital twins, and by lowering the cognitive and financial barriers to entry, the field can ensure that bionic restoration is no longer an experimental luxury/ Ultimately, the goal is to transform these devices into seamless biological extensions, restoring not just function, but a genuine sense of embodiment and independence to those living with limb loss.
Bibliography
Amin, K. R. (2022). Bionic limb replacement: an evolving concept in lower extremity reconstruction. Plastic and Aesthetic Research, 9(3), 24. https://doi.org/10.20517/2347-9264.2021.119
Azocar, A. F., Mooney, L. M., Duval, J.-F., Simon, A. M., Hargrove, L. J., & Rouse, E. J. (2020). Design and clinical implementation of an open-source bionic leg. Nature Biomedical Engineering, 4(10), 941–953. https://doi.org/10.1038/s41551-020-00619-3
Bumbaširević, M., Lesic, A., Palibrk, T., Milovanovic, D., Zoka, M., Kravić-Stevović, T., & Raspopovic, S. (2020). The current state of bionic limbs from the surgeon’s viewpoint. EFORT Open Reviews, 5(2), 65–72. https://doi.org/10.1302/2058-5241.5.180038
Cho, Y., Jeong, H. H., Shin, H., Pak, C. J., Cho, J., Kim, Y., Kim, D., Kim, T., Kim, H., Kim, S., Kwon, S., Hong, J. P., Suh, H. P., & Lee, S. (2023). Hybrid Bionic Nerve Interface for Application in Bionic Limbs. Advanced Science, 10(35). https://doi.org/10.1002/advs.202303728
Dosen, S. (2023). Toward self-contained bidirectional bionic limbs with high information throughput. Science Robotics, 8(83). https://doi.org/10.1126/scirobotics.adk6086
Freitag, K., Karayiannidis, Y., Zbinden, J., & Laezza, R. (2026). Fine-Tuning Myoelectric Control Through Reinforcement Learning in a Game Environment. IEEE Transactions on Biomedical Engineering, 73(1), 168–179. https://doi.org/10.1109/tbme.2025.3578855
Frossard, L., Conforto, S., & Aszmann, O. C. (2022). Editorial: Bionics limb prostheses: Advances in clinical and prosthetic care. Frontiers in Rehabilitation Sciences, 3. https://doi.org/10.3389/fresc.2022.950481
Frossard, L., & Lloyd, D. (2021). The future of bionic limbs. Research Features, 134. https://doi.org/10.26904/rf-134-7477
Guo, K., Lu, J., Wu, Y., Hu, X., & Yang, H. (2024). The Latest Research Progress on Bionic Artificial Hands: A Systematic Review. Micromachines, 15(7), 891. https://doi.org/10.3390/mi15070891
Long, Z., Qiu, X., Chan, C. L. J., Sun, Z., Yuan, Z., Poddar, S., Zhang, Y., Ding, Y., Gu, L., Zhou, Y., Tang, W., Srivastava, A. K., Yu, C., Zou, X., Shen, G., & Fan, Z. (2023). A neuromorphic bionic eye with filter-free color vision using hemispherical perovskite nanowire array retina. Nature Communications, 14(1). https://doi.org/10.1038/s41467-023-37581-y
Marasco, P. D., Hebert, J. S., Sensinger, J. W., Beckler, D. T., Thumser, Z. C., Shehata, A. W., Williams, H. E., & Wilson, K. R. (2021). Neurorobotic fusion of prosthetic touch, kinesthesia, and movement in bionic upper limbs promotes intrinsic brain behaviors. Science Robotics, 6(58). https://doi.org/10.1126/scirobotics.abf3368
Ortiz-Catalan, M. (2024). Thermally sentient bionic limbs. Nature Biomedical Engineering, 8(8), 938–940. https://doi.org/10.1038/s41551-023-01174-3
Ortiz-Catalan, M., Zbinden, J., Millenaar, J., D’Accolti, D., Controzzi, M., Clemente, F., Cappello, L., Earley, E. J., Mastinu, E., Kolankowska, J., Munoz-Novoa, M., Jönsson, S., Cipriani, C., Sassu, P., & Brånemark, R. (2023). A highly integrated bionic hand with neural control and feedback for use in daily life. Science Robotics, 8(83). https://doi.org/10.1126/scirobotics.adf7360
Pasluosta, C., Kiele, P., Čvančara, P., Micera, S., Aszmann, O. C., & Stieglitz, T. (2022). Bidirectional bionic limbs: a perspective bridging technology and physiology. Journal of Neural Engineering, 19(1), 013001. https://doi.org/10.1088/1741-2552/ac4bff
Schone, H. R., Udeozor, M., Moninghoff, M., Rispoli, B., Vandersea, J., Lock, B., Hargrove, L., Makin, T. R., & Baker, C. I. (2023). Should bionic limb control mimic the human body? Impact of control strategy on bionic hand skill learning. https://doi.org/10.1101/2023.02.07.525548
Schone, H. R., Udeozor, M., Moninghoff, M., Rispoli, B., Vandersea, J., Lock, B., Hargrove, L., Makin, T. R., & Baker, C. I. (2024). Biomimetic versus arbitrary motor control strategies for bionic hand skill learning. Nature Human Behaviour, 8(6), 1108–1123. https://doi.org/10.1038/s41562-023-01811-6
Song, H., Hsieh, T.-H., Yeon, S. H., Shu, T., Nawrot, M., Landis, C. F., Friedman, G. N., Israel, E. A., Gutierrez-Arango, S., Carty, M. J., Freed, L. E., & Herr, H. M. (2024). Continuous neural control of a bionic limb restores biomimetic gait after amputation. Nature Medicine, 1–10. https://doi.org/10.1038/s41591-024-02994-9
Xu, Y., Sun, Z., Bai, Z., Shen, H., Wen, R., Wang, F., Xu, G., & Lee, C. (2024). Bionic e-skin with precise multi-directional droplet sliding sensing for enhanced robotic perception. Nature Communications, 15(1). https://doi.org/10.1038/s41467-024-50270-8
Zhang, H., & Lee, S. (2022). Robot Bionic Vision Technologies: A Review. Applied Sciences, 12(16), 7970. https://doi.org/10.3390/app12167970
About the author
Sharanya Seth
Sharanya Seth is a Grade 11 student at United World College South East Asia in Singapore with a strong interest in medicine, particularly in surgical fields such as Obstetrics and Gynaecology and Plastic Surgery. She has gained early clinical exposure through internships in both Singapore and India, where she observed procedures including hysterectomies and fertility treatments, and assisted with patient interactions in a general practice setting. These experiences provided her with insight into clinical environments, patient care, and the doctor-patient relationship.
Sharanya is actively engaged in scientific research, having submitted a CREST Award project investigating the inhibitory effects of natural disinfectants such as turmeric and garlic on E. coli growth. She is currently conducting an Extended Essay exploring glucose diffusion and its relevance to diabetes, further developing her ability to apply scientific principles to real-world medical challenges.
In addition to her academic pursuits, she leads a service initiative supporting individuals with intellectual disabilities, where she organises cognitively stimulating activities to promote engagement and social interaction, as well as fosters an environment of respect and inclusivity. She also volunteers regularly at the National Kidney Foundation in Singapore, where she helps in the Dialysis Centre and Enrichment sector with patients. She has been recognised on the High Honour Roll award for three consecutive years and has achieved distinction in piano examinations, along with athletic awards.